

Viet Nam Was Once COVID-free
Now that vaccines came to visit, it isn't like that anymore.

Edit November 09, 2021:
Many people have asked for an analysis of molecular biology mechanisms that could be reasonably proposed behind this amazing set of facts shown below. It would take another mini-review that I did after first publication of these interesting screenshots below to assemble a basis for explanation.
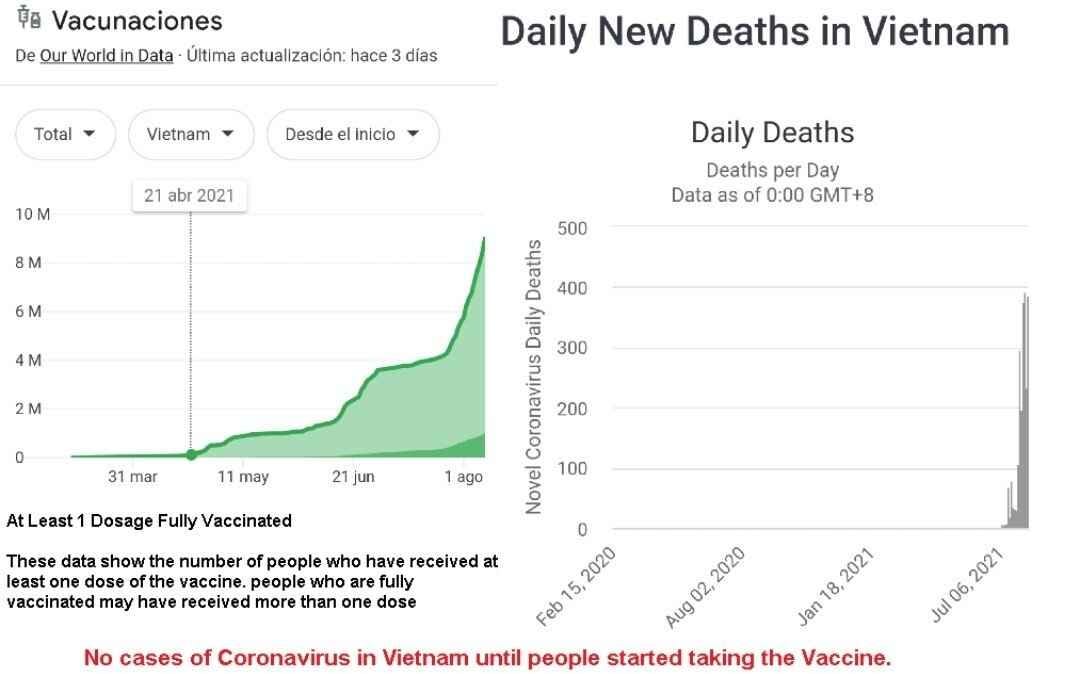
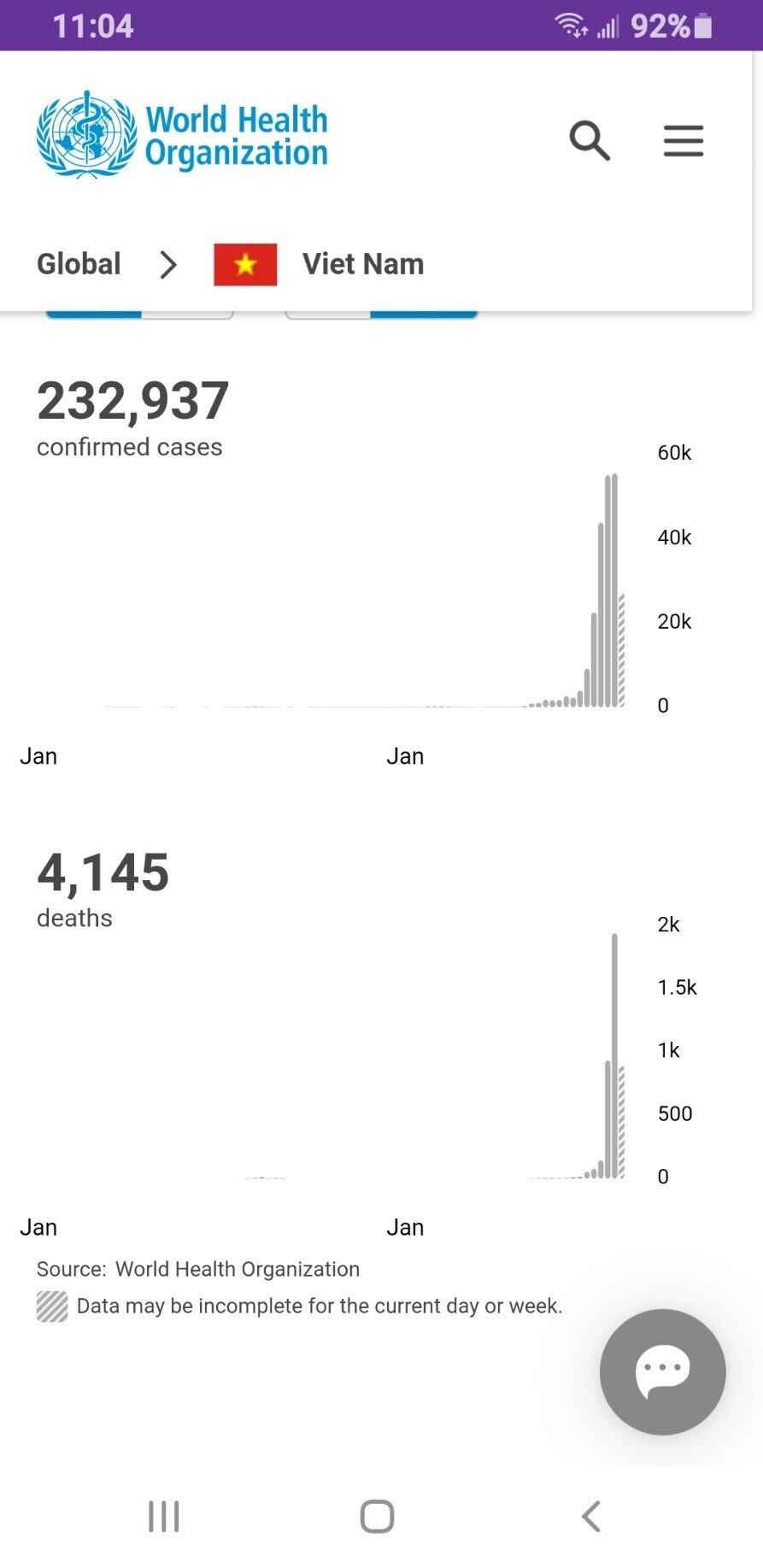
How could an impoverished equatorial country like Viet Nam go from fewer than 200 cases out of 100 million people in January 2021, literally THE WORLD LEADER in avoiding basically ALL Rona infections for a full 18 months since the globe noticed nearby China was managing a health crisis (of some kind), to being ravaged by disease in about 6 weeks starting in April? (Hint: the initials are “A”stra and “Z”eneca.) Today, Alex Berenson noticed something perhaps related, and this noticing has served as the final stimulus for my return to answer the question, because what he noticed in particular is very relevant to a good theory of where variants come from.
So here is the sudden disease theory in bolus dose:
Reverse transcription
Ubiquitous virums
Low-level viral expression
Hobbled-virus complementation
Genetic vaccines ARE helper viruses
Here is the theory restated in more detail:
Virums, particularly RNA virums, can be reverse-transcribed by our own ubiquitous reverse transcriptase enzymes, and their double-stranded DNA gene products from this process are inserted into our own genomes. The effect of this is that the inserted DNA is then forward-transcribed as messenger RNA for protein-building.
Virums are with us always, with varying levels of genetic expression (mRNA) transcribed from those genomic insertions. High-level expression of viral RNA gathers the attention of intracellular viral pattern recognizers and are eliminated, and if they go to high-copy counts of viral protein expression, the Cytotoxic T-cells of the immune system pick up on membrane-bound foreign protein products and eliminate the infected cells. Thus, there is selective pressure for virums to mutate into something passive and low-grade.
Low-level RNA transcription, with unnoticeable expression of protein products is common and important. Some of these inserted genes are probably in some way “faulty” or incapacitated, and somehow do not have the ability to assemble enough viral superstructure to mount a serious infectious disease state. An example might be a single nucleotide polymorphism (“SNP” or point mutation) that leads to a protein translational “Stop” codon, that ends a viral structural protein’s manufacture prematurely, only producing a dysfunctional fragment. Consider what that might mean if the Stop codon comes in the middle of Spike protein code.
The concept of "helper virus" is well-characterized, and they exist to co-infect in all Kingdoms of Life, including with Phage on Bacteria, infecting Plants, Protists, and us. “Hobbled” viruses can be complemented (completed) by addition of another virus that contains sufficient nucleotide sequences to re-assemble a full, restored infectious virus1.
The much-vaunted “mRNA vaccines” contain 4.2 kB (kilobases, 4,200 nucleotide bases in a strand out of 29,000 total, ~14% of the full virum) that encode SARS-2 Spike-1 protein, the engineered Wuhan virus sequence as provided originally in 2019 by the Chinese2 3 4. The upshot is that IF low-grade endemic, reasonably-closely related sarbecovirums exist in a host, AND they receive a nucleic acid vaxx, the recombination event will yield a higher copy count of a reconstituted infectious agent. In 2021 we call these agents “variants.” The nucleotide vaxx itself becomes an enabling “helper virus.”
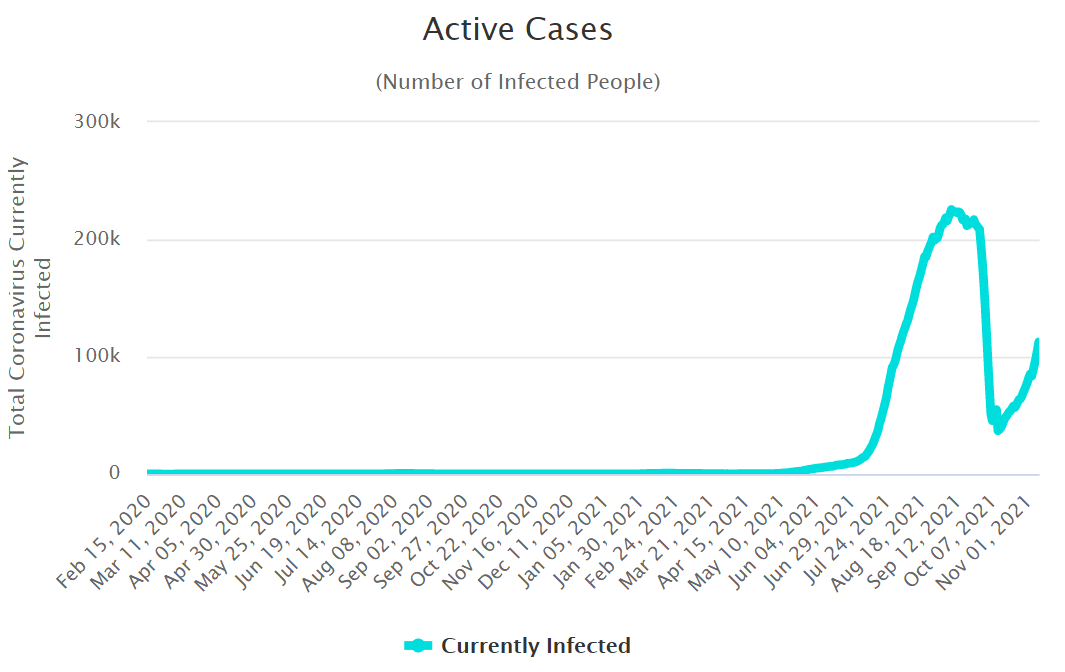
Per my other link, nearby Viet Nam neighbor Laos, harbors bats chock full of sarbecovirums. It is not unreasonable to assume that at some level throughout Southeast Asia, viruses of this type form an entire ecosystem. Their mammal-infecting propensity does not end where human civilization starts. The strong likelihood is that a critical mass of the Viet Nam population are harboring low-grade genomic viral expression and cope with that just fine. It follows that they also have low-grade endemic immunity to low levels of known local pathogens that are related to Rona. The theoretical evidence for that is simply based in the observation that the entire country was Rona-sterile until nucleotide vaccine arrived. This baseline “natural immunity” accounts for the exceptionally low Vietnamese case rate until late April 2021. By April 28th, Viet Nam reached 300+ “current infections” and has never again been that low.
As mentioned above, Alex Berenson has noticed that there are a few things off about the South Asian corridor between Pakistan and Indonesia, and he compares the U.K. Rona statistics over time to those of Pakistan, India, Bangladesh, and Indonesia.
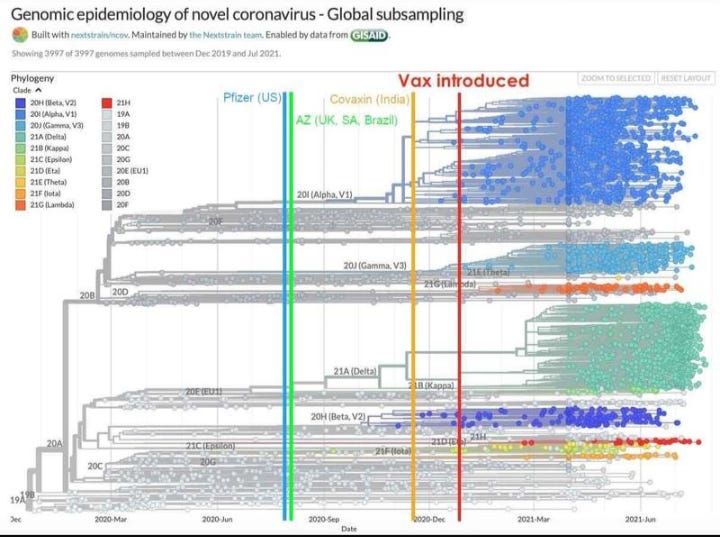
I see what effect he is attempting to demonstrate here, and the proposition is solid, but there are some quibbles: 1) A massive population fraction of Britain is Anglo-Norman/Northern European and their immunological landscape being compared with a widely disparate South Asian immunological landscape is very apples and oranges; 2) Britain, if you believe the old movies, is a “temperate zone” and this invokes concepts of seasonality and asks questions about available animal reservoirs, 3) Just looking at the 7 vaccines approved in India, some are nucleotide-expression based, yes, and their first, COVAXIN, is chemically deactivated whole virus and accounts for about 400 million jabs, according to BBC. I do not have the patience to look up the approved vaccines and currently reported fractions used in the other countries. Suffice to say that I know that AstraZeneca (COVISHIELD in India) has made major inroads in this region and their Adenovirus vector is popular. The other global pfarma companies will not leave money on the table and they will be coming along to collect theirs. Maybe not. And maybe.
If you look at the chart above, the COVAXIN date does NOT tightly correlate with the advent of India’s greatest contribution to the world so far, namely Delta Variant. But it DOES correlate within 6 weeks of the introduction date of AZ/COVISHIELD at the end of January.
The hope is that some people someplace are paying attention to what “nucleotide vaxx” is doing out there.
A popularly-known case is the Sabin “live attenuated” polio vaccine, which was a treated form of whole poliovirus that was thought to be able to enter the first few steps of the viral life cycle (oral route, through the gut, to the lumbar anterior grey roots) and generate a sterilizing immune response at the points of entry, but unable to replicate due to several damaged or removed genes, in theory. After “the Cutter Incident” it was withdrawn in the U.S. because of a manufacturing “problem” that infected kids with live wild type virums, paralyzing 200 and killing 10. After addressing the “manufacturing problem” Sabin-style virus continued to be made and then orally administered in Africa. Even recently many cases of polio developed owing to endemic low-grade polio-related coxsackie virums that are able to complement the missing genetic material of the live vaccine, recombine with the hobbled vaccine virums, and produce large amounts of fully functioning polio, leading to the paralysis and death of many African children.
See El Gato Malo’s excellent reviews of the amazing, almost superhuman, rapidity with which “science” was able to answer the call of an infected world within weeks, producing the vaxx mRNA sequences that have been in use since January 2020 and then never again updated. It was almost as if they had them at their fingertips and ready to go, but not ready to do anything new or improved in the following 2 years because what they had was something that took them years to attain.
Adenovirus vectors use DNA payloads instead of mRNA (AstraZeneca and J&J/Janssen) and then produce mRNA of their own, but persist because they insert themselves and translate just the same. The viral recombination and complementation proceed along the same paths. They, too, are based on the same China-provided engineered 2019 Wuhan strain sequence.
This modified (messenger) RNA contains a substituted nucleic acid base called N1-methylpseudouridine (m1Ψ) in place of the usual Uridine that cells use to make mRNA polymers. With m1Ψ incorporated into the strand the RNase degradation enzymes are inhibited so the vaxx protein-building signal has a longer chance to persist, in this case it has been clocked at “weeks” per a recent paper. It is also intended to blunt the response of viral nucleotide pattern recognition system causing it to mostly ignore the vaxx strand as if it is a normal mRNA product.
Will I be able to understand this post fully if I keep reading Roit?
Does this tweet thread have any bearing on what's going on?
https://twitter.com/Kevin_McKernan/status/1458274100946870275